The takeaway
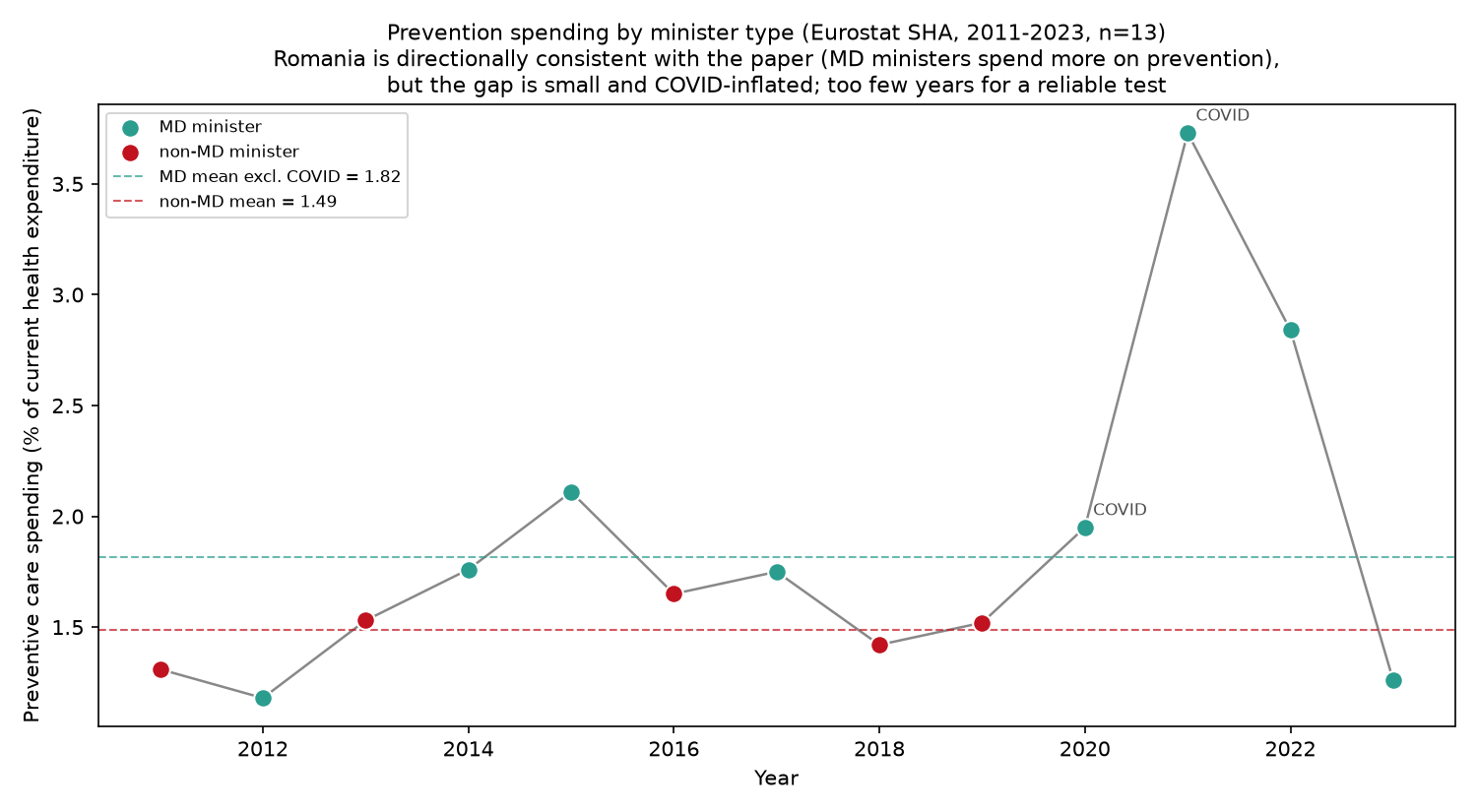
Aligned to the original paper's actual outcome measures, Romania weakly corroborates its central finding: years run by a medically-trained (MD) minister show a higher share of spending on prevention (1.82% vs 1.49% of health spending, excluding COVID) with no change in total health spending — the paper's "reallocation, not expansion" pattern.
But the signal is thin (prevention data exist for only 13 years), and a single country cannot reproduce the paper's identification strategy. This is honest descriptive corroboration — not proof of a causal effect.
01The question
The original study examines whether a health minister's clinical training shapes what a health system spends on and how it performs, across ~30 OECD countries (1993–2014) using a country-and-year fixed-effects panel. Its headline result: MD ministers don't grow total budgets — they reallocate toward preventive care (vaccines, screening), by roughly 11–14%.
Romania isn't in that sample (it isn't an OECD member), which makes it a clean out-of-sample test. We rebuilt the minister-by-minister record since 1990 and asked the same question of the same outcomes.
02What we found
Direction of the association in Romania versus the original 30-country study. Signs are comparable; magnitudes are not (different units, samples, and — crucially — identification).
| Outcome | Original study (MD effect) | Romania | Verdict |
|---|---|---|---|
| Prevention spending (% of health spending) |
+11–14% (robust) | MD 1.82% vs 1.49% excl. COVID |
consistent (weak) |
| Total health spending (% of GDP) |
no effect | no effect | consistent (both null) |
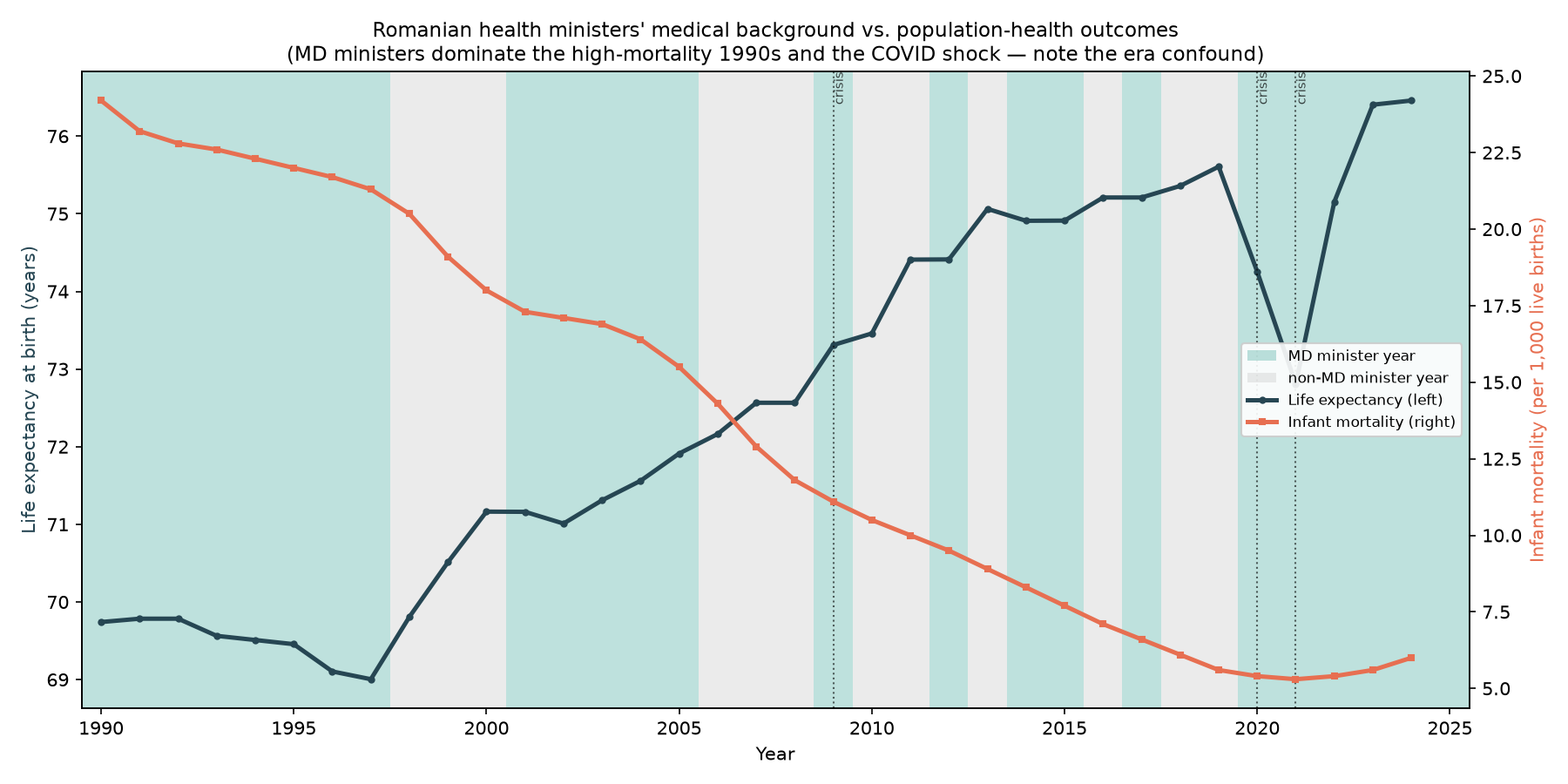
| Crude death rate | slight reduction | confounded by ageing & emigration |
inconclusive |
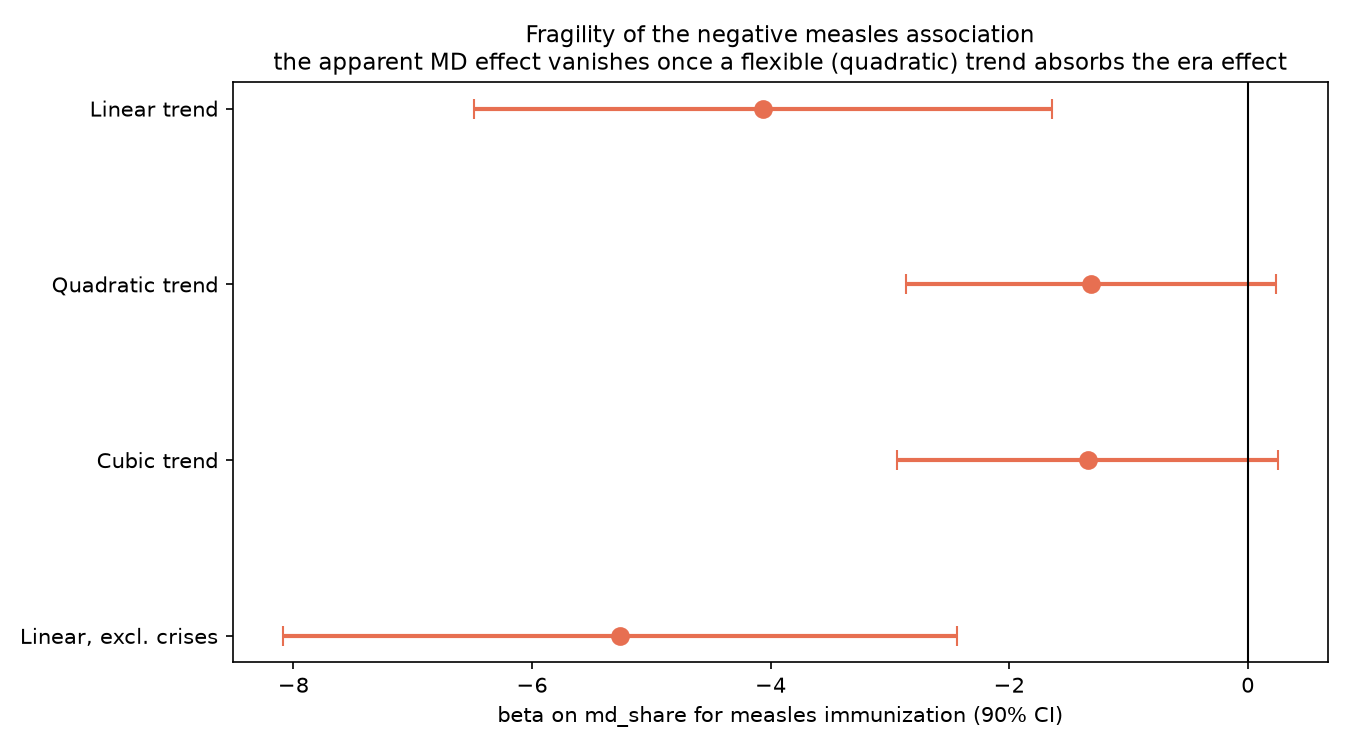
| Measles immunization | positive (not sig.) | negative overall, but positive in 1993–2014 |
mixed |
On the dimension where the original study makes its strongest claim — shifting money toward prevention without spending more overall — Romania leans the same way. Where the study relies on its multi-country panel to scrub out confounders (the death rate), Romania's single time series is dominated by demographics and can't speak.
03The evidence, in three charts
04How it was done
The data
- Ministers: 32 spells, 28 people since 1989 — hand-coded medical background, party, tenure (Wikipedia, Parliament & Ministry sources). See the full table →
- Outcomes: World Bank Open Data (spending, mortality, immunization) + Eurostat for preventive-care spending.
- Controls: government orientation, austerity years, health crises, GDP per capita, time trend.
The method
- MD-vs-non-MD year comparisons (with and without COVID).
- Time-series regressions with autocorrelation-robust errors.
- Selection & trend-fragility robustness checks.
- Fully reproducible Python pipeline; every figure regenerates from raw public data.
05What this can — and can't — say
The faithful next step is the original study's own design: a Central/Eastern European + Romania panel with country and year fixed effects. This case study is the reusable scaffolding for that larger build.